The Deprived Human Brain
By Charles A. Nelson, Elizabeth A. Furtado, Nathan A. Fox, Charles H. Zeanah
Developmental deficits among institutionalized Romanian children—and later improvements—strengthen the case for individualized care
Developmental deficits among institutionalized Romanian children—and later improvements—strengthen the case for individualized care

DOI: 10.1511/2009.78.222
In 1989, Nicolai Ceausescu, the Communist dictator who ruled Romania for 24 years, was executed by firing squad. A revolution followed, which led to a new government and then exploration by an inquisitive West of a country previously hidden from most of the world. Close to 170,000 abandoned children were discovered languishing in state-run institutions.
Most were “social orphans,” boys and girls given up by poor families. Children with medical needs were common too, abandoned because of stigma tied to their disorders or because parents couldn’t afford their care.

Mike Carroll
How did this tragedy arise? In 1966, Ceausescu decided that Romania’s surest path to power would be to increase its economic production. In his mind, that required more human capital. So Ceausescu outlawed contraception, forbade abortion and taxed families who produced fewer than five children. The birthrate skyrocketed and poverty radiated. Because many families could not afford to keep all the children they were coerced into having, Ceausescu expanded a network of institutions where the state vowed to raise abandoned children. Rather than being stigmatized, child abandonment became implicitly endorsed, a cultural shift in Romania. Increasing numbers of children were brought to institutions early in life. Parents retained legal ties to their children and some visited. A fair number, however, simply disappeared from the lives of their infants and children.
Shortly after the 1989 coup, Western media documented horrific conditions in these institutions. Young children were found confined in cribs with filthy bedding and little sensory stimulation. In any given institution, the ratio of young children to “caregiver” might be 15 to one. Staff often had little education and no training in child development. Regimentation ruled. Children were simultaneously placed on rows of plastic pots for toileting, wore similar haircuts (regardless of gender), were dressed alike and were fed on schedule, in a largely silent, mechanical manner. Nutrition was inadequate. In some institutions, older children were physically or sexually abused.
In 2000, our research team began assessing young children in Romanian institutions. By then, the institutions had improved significantly and remained, in the minds of many, acceptable destinations for very young children. By assessing these children, however, we documented multiple ways that institutional life can hinder normal brain development in young children. We also observed how children improve after they are placed in quality foster care. The findings encouraged changes in Romania but have much wider implications. Governments worldwide, we have concluded, should not wait too long before finding good homes for the millions of children estimated to be living in institutions worldwide today.
After the plight of Romania’s institutionalized children was revealed, parents in the West rushed to help. Thousands of orphans were adopted into homes in the United States, Great Britain and Canada. But many parents soon found themselves overwhelmed by their Romanian children’s special needs. Many of these children were very small for their age. They displayed significant cognitive and language delays, behavior problems (particularly hyperactivity) and perhaps most noticeably, problems forming and maintaining relationships with significant others. Fortunately, for many, the worst problems resolved. But difficulties with interpersonal relationships and with so-called executive functions (including the regulation of attention and emotion) persisted.
Should we have been surprised at these behavioral sequelae? No. It has been known since the middle of the 20th century that children reared in institutions are characterized by delays in most developmental domains, including physical growth and cognitive, linguistic and emotional development. Such children frequently experience difficulty regulating attention and emotions. Many are indiscriminate in social encounters. For example, they might climb on the lap of one complete stranger or walk away with another. The longer children remain in institutions, the more likely they are to be developmentally delayed or challenged, earlier research showed.
Despite a known association between institutional rearing and poor developmental outcomes, uncertainty persisted as to why. Abundant research with animals (particularly monkeys) has underscored deprivation’s effects. Harry Harlow of the University of Wisconsin conducted landmark studies in the 1950s that demonstrated ways that infant monkeys reared without their mothers suffered significant emotional damage. But researchers wondered whether institutional rearing truly was to blame. Perhaps children abandoned to institutions, the thinking went, differ from those who are not. For example, perhaps they experienced more prenatal complications, or the children were born with higher incidence of genetic defects (Down Syndrome, for example) or perinatal complications such as cerebral palsy. Perhaps their families were poor and that explained it.
On the other hand, some researchers wondered if studies actually underestimated institutionalization’s effects on child development. In studies of children adopted from institutions, for example, there is a significant potential for sample bias. It could be that only the healthiest or best-looking children get adopted. Adoption studies involving only those children—which have reported substantial development gains—may have underreported physical and cognitive developmental problems overall. To address these and other questions, in 2000 we launched a scientific and humanitarian undertaking called the Bucharest Early Intervention Project (BEIP). Still underway, BEIP is a randomized, controlled trial of foster care as an intervention for children institutionalized in Romania. The project recruited participants from all six institutions for young children in Bucharest and conducted baseline assessments of 136 children and their caregiving environments. The children selected were all relatively healthy, with no obvious chromosomal disorders or major handicapping conditions such as cerebral palsy or fetal alcohol syndrome.
Half the children were then randomly assigned either to high-quality foster care created specifically for the study or to care as usual, meaning continued institutional care. The average age at foster care placement was 22 months (with a range of 6 to 31 months). Following randomization, the children were assessed again at 30, 42 and 54 months, with development of children in foster care compared to children still in institutions. For further comparison, we also assessed a group of never-institutionalized Romanian children recruited from pediatric clinics. Each time, we measured the children’s physical growth, cognitive function, social and emotional development, attachment, and problem behaviors. We also measured aspects of language development, the caregiving environment, psychiatric symptoms and brain functioning. We have reported some of the results in the scientific literature over the past six years and are currently reevaluating children as they reach eight years of age. Before detailing our findings, we feel it is important to review a number of ethical issues we grappled with and to spell out the intellectual framework that informed this research.
Because abandoned infants and toddlers living in state-run institutions are extremely vulnerable, we exercised tremendous caution with the Romanian children. One can reasonably question the ethics of even conducting a randomized study in which half the children enrolled would receive care already considered inferior. It is important to understand that when we began, there was almost no government foster care available in Bucharest. Government care for abandoned children still took the form of institutionalization. There was a debate within the government about whether institutional care or foster care was preferred. In addition, no randomized, controlled trial had ever compared foster care and institutional care, meaning that no clear conclusions could be made about their differences. Previous studies were all suspect due to potential sample bias. It was in this context that Romania’s Secretary of State for Child Protection invited us to conduct the study.
We were motivated, in part, by the fact that all of the children would likely have remained institutionalized if the study weren’t pursued. We insisted that no child whom we placed in foster care would ever be returned to an institution. We did not require any children to remain in institutions for the length of the study. In fact, as the study progressed, most children randomly selected to remain in institutions were reunited with their families, adopted domestically or placed in government foster care that did not exist at the time the study began. Indeed, of the 68 children originally assigned to care as usual, only 14 remain in institutions at this writing.
To understand why institutional care harms children, it is vital to understand the needs of a developing human brain. It is true that genetics plays an important role in postnatal brain development. But experience is the engine that drives much of that development. If children don’t have certain experiences, their brains may not develop to their full potential. A second vital principle is that many aspects of sensory, cognitive, language and social-emotional development depend on experiences occurring during particular time periods—so-called sensitive periods. Should stimulation be absent during those periods, development can be compromised significantly and, in some cases, permanently.
Stephanie Freese
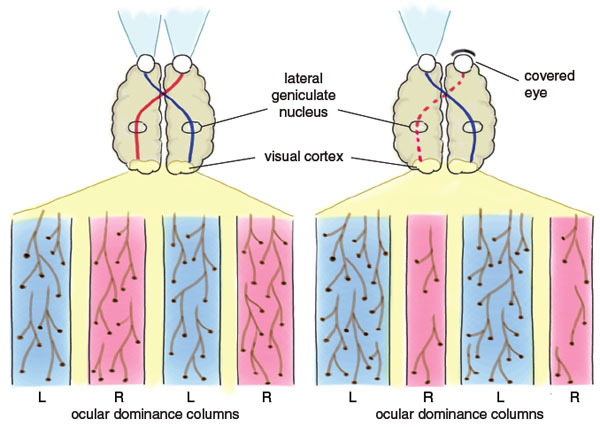
Consider this example: The ability to see the world in three dimensions using both eyes—binocular, or stereoscopic, vision—is predicated on an infant’s ability to move his or her eyes together to converge on a distant object or scene. For children whose eyes are crossed or in whom one eye lacks the ability to move in coordination with the other, the risk of failing to develop binocular vision is great. If this condition is treated in the first few years of life, normal vision can be restored. But if there is no treatment or an attempted treatment fails, the child will never develop binocular vision.
We now understand a great deal about the neurobiological mechanisms that underlie sensitive periods. As a general rule, synapses (points of contact between neurons) are massively overproduced in newborns, who have many more synapses than adults. Over time, synapses are lost, or pruned, a process that is heavily dependent on experience. In the case of binocular vision, experiments involving cats showed that input from the two eyes is sent to columns of related cells that reside in the visual cortex. The cells and synapses that make up these ocular dominance columns get pruned over time at rates based on the input they receive from the two eyes. If the input is below normal, the pruning is above normal, since some synapses are not adequately stimulated or “confirmed.” If normal input is not restored during a sensitive period, the opportunity to establish binocular vision is lost.
Sensory and social deprivation function similarly. Imagine that a baby’s eyes are fine, but the infant has little or nothing to look at. That occurs when infants lie on their backs in cribs facing a white ceiling and remain there for the first year or more of life, except for the occasional feeding. Instead of seeing a rich and changing visual world composed of patterns and color and form, they see a relatively static, patternless and achromatic world.
In many (but not all) institutions, children can be deprived of much more than patterned light information. Because they are rarely held, infants can receive little tactile input. Since a single caretaker may look after 15 or more children, language and cognitive stimulation are minimal. Perhaps most importantly, since many children do not get the opportunity to form a deep and lasting relationship with a primary caregiver, both their social and emotional development can be compromised. Previous studies, although deficient as previously described, do suggest some neurobiological differences among institutionalized children. Tests have found reduced metabolic activity in regions of the children’s frontal cortex, which is involved in executive functions such as planning and emotional regulation, and in the temporal cortex, involved in memory, language and emotion. Reduced connections between the brain regions also were detected.
Our project in Romania allowed us to assess the effects of general deprivation on many aspects of development. We also could ask whether the toll of early deprivation can be reversed by intervention. And we could hunt for sensitive periods, a line of inquiry that we hoped could help elucidate which experiences must occur at what time in order to facilitate normal development.
In virtually every domain we measured, developmental deficits were observed among institutionalized Romanian children. We’ll begin with attachment. Healthy feelings of attachment between an infant and at least one adult are vital to a child’s ability to pursue healthy relationships throughout life. In Romania, we assessed attachment using the Strange Situation Procedure. This protocol includes a series of interactions including separations and reunions between an infant, a parent or caregiver and an adult stranger. Institutionalized children were paired with caregivers they were observed favoring. The moderately stressful procedure assesses the child’s balance between exploratory behavior and seeking closeness and comfort from a parent/caregiver rather than a stranger.
Stephanie Freese
Trained graduate students and faculty, unaware of which children were institutionalized, observed video recordings of the children’s behavior during those encounters and classified it as “secure,” “insecure” or “disorganized.” The latter category describes young children who display contradictory or confused attachment behaviors or display fear of the caregiver. Disorganized attachment is often an indicator of increased risk of current and future psychopathology in children. Coders also rated the degree to which attachments between a child and a caregiver had formed at all.
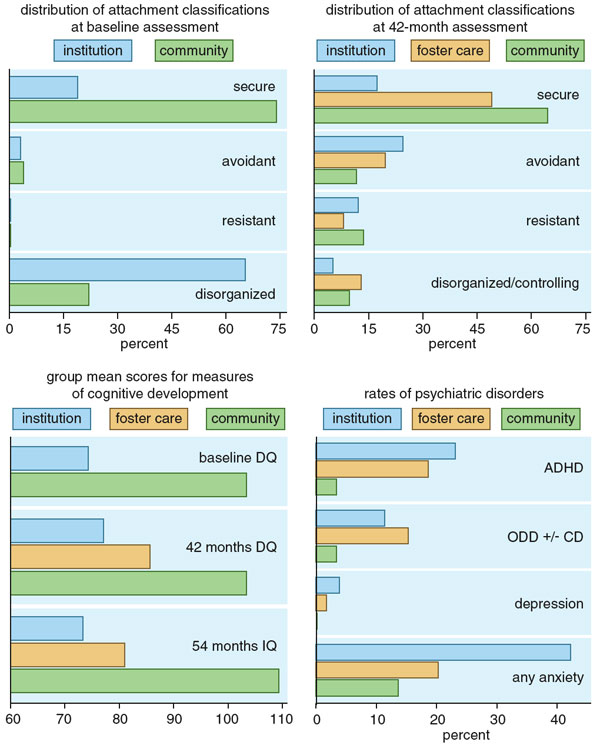
The assessment results were powerful. We found that 100 percent of the attachments of the never-institutionalized children were rated as being fully developed, but only 3 percent of the institutionalized children had fully formed attachments. Prior to randomization, 65 percent of the institutionalized children had a disorganized attachment with their favorite caregiver, and another 13 percent had so little attachment behavior that they could not even be classified. In contrast, only 22 percent of the never-institutionalized children living with their families had disorganized attachments to their mothers.
We also screened for reactive attachment disorder (RAD), including children displaying emotionally withdrawn or inhibited behaviors, and children who were indiscriminately social or disinhibited. The former fail to seek out or respond differentially to adult caregivers, display impaired social engagement and reciprocity and have trouble regulating their emotions. The latter lack selectivity when seeking comfort and support, engage with unfamiliar adults, fail to check back with caregivers in unfamiliar settings, and are willing to approach, interact with and go off with complete strangers. The institutionalized children in Romania demonstrated significantly higher levels of RAD compared to children in the never-institutionalized group.
In assessing the children’s caregiving environment, we used a tool called the Observational Record of Caregiving Environment. We videotaped subjects in their home environments with their preferred caregiver for 1.5 hours. These videotapes were subsequently coded for caregiver and child behaviors. A caregiving quality score was obtained by averaging five qualitative scores (caregiving sensitivity, stimulation of development, positive regard for child, flat affect and detachment). As we expected, caregiving quality scores were higher among children living with their families than among children living in institutions.
The Bayley Scales of Infant Development was used to evaluate cognitive development in the BEIP sample at the start of the study, before any children were placed in foster homes, and later at age 30 and 42 months. Children reared in institutions showed greatly reduced intellectual performance compared to children raised with their biological families. Mean Bayley Mental Developmental Index (DQ) scores, roughly equivalent to Intelligence Quotient (IQ) scores, were 74 for children in the institutionalized group at 30 months, a level associated with mental retardation. They were 103 for children in the community group, which is perfectly average.
Perhaps one of the most unusual characteristics of this research is the measurement of brain activity in infants and young children. To our knowledge, the BEIP is the only study that has measured brain activity in infants and young children while they lived in institutional settings. Brain activity was measured by recording the electroencephalogram (EEG) and its subset, the event-related potential (ERP). Children were fitted with a Lycra stretch cap (much like a swimmer’s cap) that contains small sensors that permit us to record electrical brain activity.
The EEG was recorded from 15 electrodes during an activity designed to elicit quiet attention in infants and young children. EEG power (a proxy for the amount of brain activity) in three frequency bands (3–5 hertz as theta, 6–9 hertz as alpha, 10–18 hertz as beta) was computed at each electrode site. Each frequency band is assumed to possess a different functional significance. Alpha activity, for instance, generally reflects a conscious state of mind with associated cognitive processing; beta activity generally reflects a more active engagement with the environment. During baseline testing, children in the institutionalized group showed lower alpha and beta power compared with the group of age-matched children living in the community. The pattern of findings suggests a delay in brain development among the institutionalized children.
The ERP represents the brain’s amplitude and pace of response to the presentation of a distinct event. ERPs were recorded in response to facial expressions of fear, anger, happiness and sadness. We examined both the peak amplitude (magnitude of the brain response signal) and latency (time at which the response signal occurred) of various ERP components whose functional significance has been well documented in the research literature. Several differences were observed between children living in institutions and those living in families. Amplitudes were smaller for several ERP components in the institutionalized group compared with the community children. Second, latencies for these components were longer in the institutionalized group, indicating slower processing in children with a history of institutionalization. Finally, children in the never-institutionalized group demonstrated right-hemispheric specialization for faces, the expected response. Children in the institutionalized group simply did not.
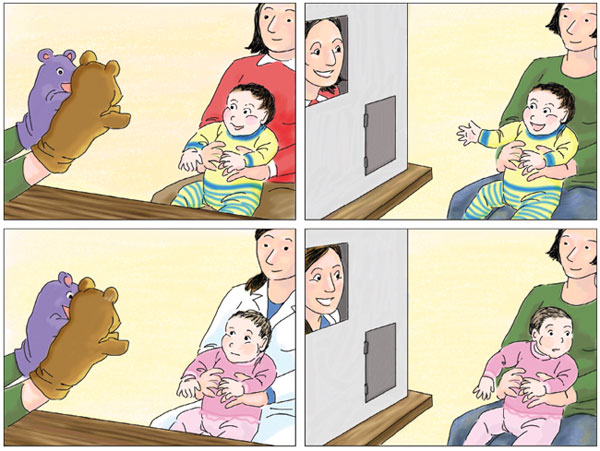
The children also engaged in two tasks from a standardized emotion reactivity assessment battery called the Lab-TAB. These two tasks, puppet play and peek-a-boo, were designed to elicit positive emotional responses in young children. For the puppets task, a child was seated on his or her caregiver’s lap and presented with two puppets that talked to each other and the child and later attempted to tickle the child. In the peek-a-boo task, the child was seated on the lap of a research assistant and watched as the child’s parent or caregiver played peek-a-boo through a wooden screen. The sessions were videotaped and subsequently coded for the child’s facial expressions, vocal behaviors and attention. Children living in institutions displayed significantly fewer positive emotions, significantly more negative emotions and less attention compared to typically developing Romanian children living with their parents.
Our findings were not all bleak. Children’s fates, our results to date argue, are not sealed if they are temporarily institutionalized. In almost every domain we evaluated, children placed in foster care made significant developmental gains when compared to children who remained in institutions. It is important to note that the children were placed in quality foster care settings. Foster parents were paid, trained and encouraged to develop loving, committed relationships with the previously institutionalized children. Sympathetic social workers visited the foster parents, who also had access to support groups.

Mike Carroll
A good place to observe improvement is with attachment testing performed at 42 months. The Strange Situation Procedure was repeated, and episodes were coded using a preschool coding scheme. This time, 49 percent of children placed in foster care demonstrated secure attachments as compared to 18 percent of children in the institutionalized group. Among children living with their parents in the community, 65 percent were securely attached.
Children placed in foster care had large reductions in signs of emotionally withdrawn or inhibited RAD at 30 months of age; their scores were indistinguishable from the community children sample at every age we assessed. The reductions in signs of indiscriminately social or disinhibited RAD behavior were less dramatic, however. Only at 42 months did children in foster care score lower than children in the institutional group.
Cognitive development was reassessed at 54 months using the Wechsler Preschool Primary Scales of Intelligence, a test more appropriate for that age group. Children in foster care experienced significant gains in cognitive function compared to children in the institutional group. At that point, the mean IQ was 81 for children in foster care compared with 73 for institutionalized children and 109 for the remaining children.
Also, the Lab-TAB tasks, those puppets and peek-a-boo protocols, were readministered at 30 and 42 months of age. Children taken out of institutions and placed in foster care displayed more positive emotions and paid better attention than children who remained institutionalized at 30 and 42 months.
Stephanie Freese
Similar improvements were observed in the children’s language development and their vulnerability to psychiatric symptoms. Children who were institutionalized and children placed in foster care for only a brief period showed substantial language delays by age 30 or 42 months. Some were not yet producing intelligible words. Children in foster care for at least one year matched the expressive output and receptive language of children living in the community, but they demonstrated lower expressive grammatical abilities. Children in foster care exhibited significantly fewer emotional disorders, such as anxiety, than children in the institutionalized group.
Psychiatric symptoms cannot be reliably diagnosed in very young children. So we waited and assessed the children at 54 months, using the Preschool Age Psychiatric Assessment, a structured psychiatric interview of parents and caregivers. The assessment evaluates school and day care functioning, family structure and functioning, parenting behaviors and a host of demographic variables. Among the children who had lived in institutions, 55 percent had diagnosable psychiatric disorders at 54 months. By contrast, only 22 percent of children in the community met criteria for a disorder.
Compared to the community group, the institutionalized and foster children had higher levels of emotional disorders (including anxiety and depressive disorders) and behavioral disorders (including attention deficit hyperactivity disorder, ADHD; oppositional defiant disorders; and conduct disorder). Removing children from institutions did not make them immune to all difficulties, however. There was no evidence that the intervention reduced behavioral disorders such ADHD, a puzzle that may not be solved until science better understands the mechanisms underlying that disability and when those mechanisms emerge. The need is urgent, since ADHD harms people’s ability to learn throughout life and can increase the risk of being impulsive, which can result in poor decision making. The developmental psychopathology literature suggests that “externalizing” disorders, those involving behaviors, likely begin in children earlier than “internalizing” disorders, such as depression and various anxiety disorders. Boys are believed to be at higher risk.
As we have reported in Science, the improved cognitive outcomes for children in foster care that we observed at 42 and 54 months were most significant for children placed into foster care before 24 months of age. These children had higher DQ and IQ scores than children placed in foster care after 24 months.
Similar sensitive periods were observed in language, attachment and indiscriminate behavior. For language, children placed into foster care before the age of 15 months exhibited better language abilities at 30 and 42 months than children placed into foster care after the age of 15 months. Children placed in foster care before 24 months of age demonstrated more secure attachments at 42 months than children placed in foster care after 24 months. The earlier children were placed in foster care, the less likely they were to show disorganized attachments. Though the age cutoffs vary across domains, our results strongly support intervention at earlier ages.
This research has had an impact in Romania. After learning of our preliminary findings, the government there passed a law forbidding the institutionalization of children younger than two years old unless a child was severely handicapped. Now only 30,000 children remain in institutions. The BEIP findings also have implications for orphaned or abandoned children around the world. A common societal response is to place such orphaned or abandoned children in institutions.
Our study questions this practice, especially for countries positioned to use foster care as an alternative. And it speaks forcefully to the importance of removing children from institutions as early as possible and, ideally, placing them in families equipped to nurture them. We see implications too for young children at risk of neglect or abuse while living with their families, in the United States and elsewhere. Progress made by Romanian children placed in foster care makes a case that adverse early experiences need not have lifelong effects. But if young children remain in neglectful or abusive homes for too long, the risk of longterm harm may be too great. Temporary placement while parents seek remediation might be a better course. Over time, as we reassess these Romanian children as they grow older, they may teach us more about what children’s brains need and when they need it most—no matter where they live.
Click "American Scientist" to access home page

American Scientist Comments and Discussion
To discuss our articles or comment on them, please share them and tag American Scientist on social media platforms. Here are links to our profiles on Twitter, Facebook, and LinkedIn.
If we re-share your post, we will moderate comments/discussion following our comments policy.